Hypoxia in Aviation: A Pilot's Perspective
Hypoxia: Legal, Subtle, and Easy to Miss
Hypoxia in aviation is one of the most insidious threats to pilot safety, yet it’s often misunderstood as simply an altitude problem. Hypoxia is one of those aeromedical topics that pilots tend to “know,” at least academically. We memorize altitude thresholds, learn the regulatory oxygen requirements, and can usually recite the symptoms on demand when requested. What is less intuitive, and far more important operationally, is how quietly hypoxia can degrade performance, and how easily it can do so while we remain within the regulations.
A flight I made last December reinforced that lesson for me in a way no textbook ever has.
A Legally Sound Plan
I needed to make a short hop over the Sierra Nevada, transiting near the Mount Whitney area with a descent into Lone Pine (O26). The plan was conservative in the ways most pilots think about: favorable weather, known route, and performance margins that supported a brief ridge crossing followed by a rapid descent.
To minimize exposure to higher altitudes, I delayed the climb as long as possible, crossed the ridge efficiently, and planned to descend promptly on the east side. The time spent just under 13,500 feet would be well below the 30-minute limitation that allows flight without supplemental oxygen under 14 CFR 91.211.
From a regulatory standpoint, the plan was compliant. From a systems standpoint, the aircraft was operating normally. Nothing about the situation felt rushed or unsafe.
The Moment That Didn’t Make Sense
As I cleared the last peak and began setting up for the arrival into Lone Pine, I tuned in the ATIS. The broadcast included winds reported as “160 at 10.”
That information should have been immediately actionable. Determining the appropriate runway based on wind direction is a basic task that normally happens almost automatically. Instead, I found myself stuck, replaying the phrase in my head.
I remember thinking: Does that mean I land on Runway 16? Or the opposite? I wasn’t panicked, disoriented, or physically uncomfortable. I just couldn’t reason through something that should have required almost no mental effort.
Nothing dramatic happened. The flight continued normally and I landed safely. But that moment stood out precisely because it was so subtle and so abnormal for me.
In hindsight, it was a mild but clear example of hypoxia.
Understanding Hypoxia in Aviation
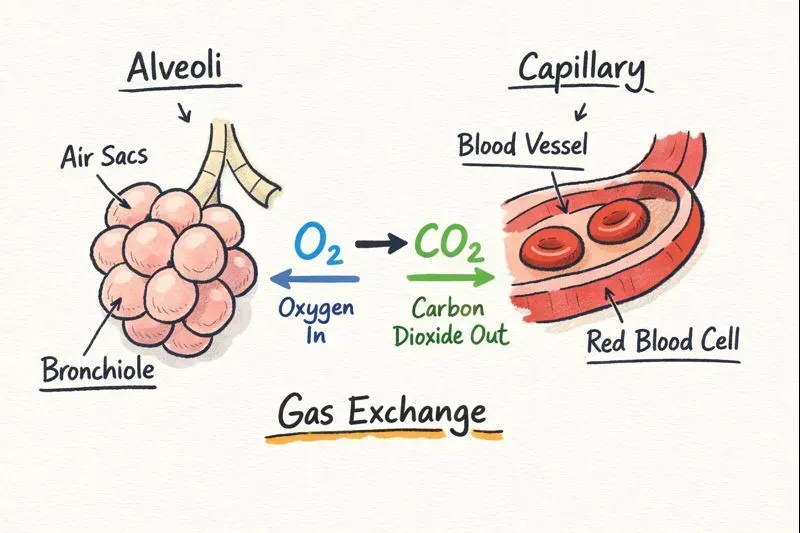
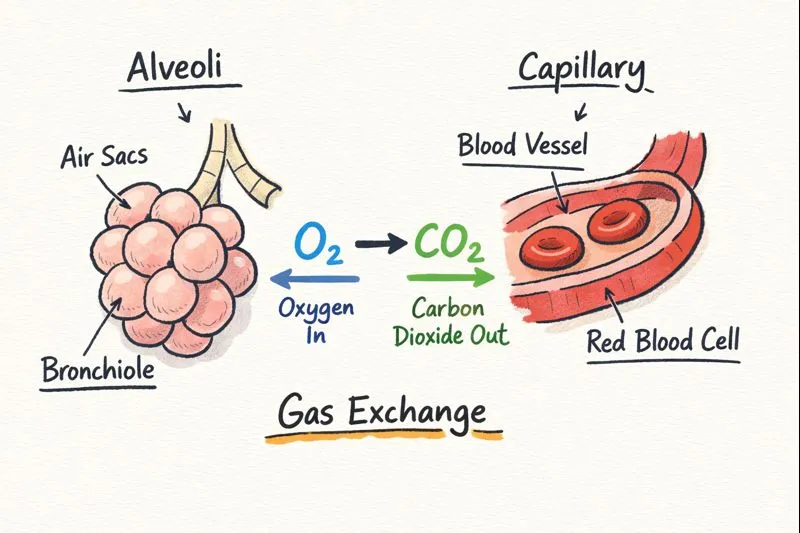
One of the most persistent misconceptions about hypoxia is that it involves a lack of oxygen in the air. In reality, the percentage of oxygen in the atmosphere remains essentially constant at about 21 percent, whether you are at sea level or at 18,000 feet.
The issue is not oxygen concentration, but rather it is partial pressure.
As altitude increases, atmospheric pressure decreases. With lower pressure, fewer oxygen molecules are available in each breath, and the pressure gradient that drives oxygen from the lungs into the bloodstream is reduced. Even though you are breathing the same percentage of oxygen, less of it is able to cross into the blood and ultimately reach the brain.
This is why hypoxia is fundamentally a pressure problem, not a composition problem.
The Physiology: Why the Brain Is First to Suffer
The human brain is particularly sensitive to reductions in oxygen availability. It accounts for only a small percentage of body weight, but it consumes a disproportionate amount of oxygen. When oxygen delivery drops, the brain prioritizes basic survival functions over higher-order cognitive processes.
That means judgment, reasoning, short-term memory, and decision-making are often the first abilities to degrade. Importantly, this degradation can occur well before physical symptoms like shortness of breath or dizziness become noticeable.
From an operational standpoint, this is what makes hypoxia so dangerous. The very tools we rely on to detect a problem, self-assessment and judgment, are the first ones to be impaired.
The Types of Hypoxia: A Review
While altitude-related hypoxia gets the most attention in aviation, it is only one of several forms pilots should understand.
Hypoxic hypoxia is the type most commonly associated with altitude. It occurs when reduced atmospheric pressure limits the amount of oxygen available for gas exchange in the lungs. Examples of when you should be alert for this type of hypoxia include 1) high terrain crossings, 2) extended time above 10–12k feet and 3) night flying at moderate altitude.
Hypemic hypoxia occurs when the blood’s ability to carry oxygen is compromised. Carbon monoxide exposure is the most common aviation-related cause. CO binds to hemoglobin far more readily than oxygen (about 200x!), effectively crowding oxygen out, even when oxygen levels in the lungs are normal. Examples to look out for are exhaust leaks in cabin heaters. You can combat this type of hypoxia by having a good CO detector in the flight deck, and please, not one of the CO-reactive “dot” detectors.
Stagnant hypoxia results from inadequate blood flow. This can occur in high-G environments, with prolonged immobility, or in cold conditions where circulation is reduced.
Histotoxic hypoxia occurs when the body’s cells are unable to use oxygen effectively. Alcohol (even the night before!), certain medications, and some toxins can contribute to this form of hypoxia. In these cases, oxygen may be present and delivered, but the cells cannot metabolize it properly.
The common thread across all types is impaired oxygen delivery or utilization at the tissue level, particularly in the brain.
Remembering the types of hypoxia are as easy as knowing your ABCS! The acronym maps directly to the oxygen pathway
-
Altitude (Hypoxic) — can you get oxygen into the lungs?
-
Blood (Hypemic) — can you carry it?
-
Circulation (Stagnant) — can you move it?
-
System (Histotoxic) — can cells actually use it?
Why Hypoxia Rarely Feels Dangerous
Hypoxia does not trigger a reliable pain response. There is no built-in alarm that clearly signals “low oxygen.” Instead, the onset is often gradual, and the symptoms are subtle: slowed thinking, fixation, mild euphoria, or misplaced confidence.
In my case, the symptom wasn’t confusion in a dramatic sense. It was a slight delay in reasoning, just enough to be noticeable. That’s typical. Many pilots who experience hypoxia report feeling capable, calm, and even confident—right up until performance begins to suffer.
This is why hypoxia is often described as insidious. It doesn’t feel like an emergency. It feels like everything is normal, just slightly dulled.
Night Operations and Hypoxia
Night flying deserves special mention because hypoxia affects night vision at much lower altitudes than it affects daytime visual acuity.
The retina’s rod cells, which are responsible for night vision, are extremely sensitive to oxygen deprivation. Studies and operational experience have shown that night vision degradation can begin as low as 5,000 feet MSL, well below altitudes where pilots typically consider oxygen use.
Reduced night vision can lead to difficulty detecting traffic, terrain, and unlit obstacles, even when the pilot otherwise feels fine. Fatigue, smoking, and mild hypoxia can compound each other, further degrading visual performance.
From an ADM standpoint, this means that night operations at moderate altitudes deserve a higher level of conservatism than daytime flights under similar conditions.
ADM: Beyond Legal Compliance
This flight reinforced an important ADM principle: regulatory compliance is not the same as optimal performance.
The oxygen regulations are minimum standards designed to accommodate a wide range of pilots and conditions. They are not guarantees of unimpaired cognition. Individual susceptibility to hypoxia varies significantly, and factors such as fatigue, dehydration, illness, and workload can all lower tolerance.
Better ADM involves asking not just, Is this legal? but Am I setting myself up for maximum cognitive performance?
What I Could Have Done Better
There were several opportunities to improve the margin:
-
Use supplemental oxygen earlier, even though it was not legally required. Oxygen is a performance tool, not just an emergency measure.
-
Plan for human performance, not just aircraft performance, when operating in high-terrain environments.
-
Treat subtle cognitive delays as meaningful data, rather than dismissing them.
-
Recognize the compounding effects of altitude, workload, and environmental factors.
None of these changes require dramatic procedural adjustments. They reflect a mindset that prioritizes capability and margin.
The Value of Hypoxia Awareness Training
One of the most valuable aspects of altitude chamber training, such as the FAA’s PROTE program, is learning your personal hypoxia symptoms. Textbook descriptions are helpful, but recognition under real conditions depends on understanding how hypoxia manifests in you.
When judgment is compromised, recognition has to be automatic. That only comes from experience and training.
Final Thoughts
Every pilot needs to understand hypoxia in aviation operations. Whether flying unpressurized aircraft above 10,000 feet or making decisions about oxygen use, recognizing the subtle signs of hypoxia can mean the difference between a safe flight and a dangerous situation. Hypoxia is rarely sudden or dramatic. It is quiet, progressive, and often masked by a sense of normalcy. That is precisely why it deserves deliberate attention in both training and operational decision-making.
This flight wasn’t about a bad decision—it was about recognizing that there was room to make a better one. Good ADM is not about perfection; it’s about continuously refining how we manage risk, especially human-factor risks that don’t announce themselves.
Being legal got me across the mountains. A more conservative approach would have given me a sharper mind while doing it.
Follow-Up: Experiencing Hypoxia Firsthand
After publishing this article, I had the opportunity to experience hypoxia firsthand inside the FAA’s Portable Reduced Oxygen Training Environment (PROTE) during a training event at San Carlos Airport. The experience was eye-opening and reinforced many of the concepts discussed here.You can read about that experience in the follow-up article: Inside the FAA Hypoxia Chamber: What Hypoxia Actually Feels Like for Pilots.
David Stites, MEI
Multi-engine flight instructor and professional ferry pilot in the San Francisco Bay Area.
Ready to Start Your Multi-Engine Training?
Contact me today to discuss your training goals and schedule your first lesson.
Get in Touch